|
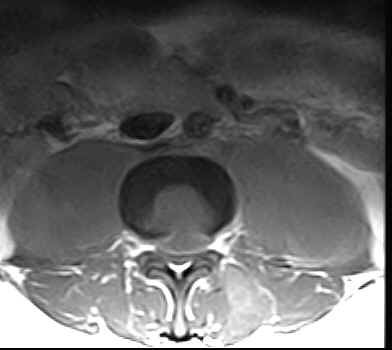
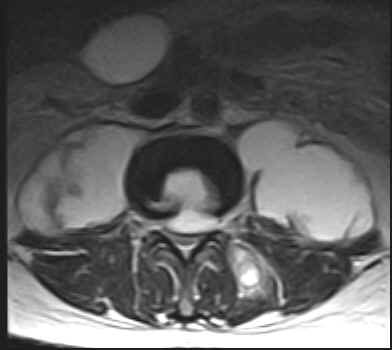
The L1, L2 and
L3 vertebral bodies show hypointense areas on the T1W images and
these turn hyperintense on the T2W images. The L1-L2 and L2-L3
intervertebral discs are also involved. There is an anterior
epidural lesion at the L2 and L3 vertebral levels. It is
hypointense with a hyperintense rim on the T1W images and
hyperintense with a hypointense rim on the T2W images. This
would be suggestive of an abscess. Slight prevertebral soft
tissue extension is noted. The psoas muscles are bulky
bilaterally and show presence of abscesses. A similar lesion is
noted within the left paraspinal muscles.
On MRI:
·
There is replacement of the normal marrow by inflammatory tissue
(with hyperemia, edema and pus) and this is usually hypointense
on the T1W images and turns hyperintense on the T2W images. It
may be found in the subchondral region or may be seen as a more
diffuse involvement. The sagittal images may show it to be a
disc centered process. Contrast enhancement is useful in those
who have an inhomogeneous marrow pattern and is of marginal
value in those with fatty vertebral marrow. Fat saturation
techniques help. Typically the hyperemic and osteomyelitic bone
enhances. Skip lesions may be seen with multivertebral
involvement and relative sparing of the intervertebral discs.
Involvement of the posterior elements is fairly common.
·
In people over thirty years an intranuclear cleft (hypointense
linear signal on the T2W images) is noted within the centre of
the disc. The loss of this cleft on T2W images may suggest early
discitis (especially when the cleft is well visualized within
the other discs). The disc may be decreased in height and
hyperintense on the T2W images. Occasionally an enlarged
edematous disc may be encountered. Adjacent marrow signal
changes and erosion of the cortical endplates may be seen. The
involved disc has a very variable pattern of enhancement.
Initially thin central linear or thick focal enhancement
conforming to the signal alteration on the T2W images may be
seen. Thin or thick marginal disc enhancement may be noted.
Occasionally the disc enhances inspite of there being no signal
alteration.
·
Tuberculosis tends to involve the soft tissues commonly with
abscess formation. Large paravertebral or psoas abscesses
(calcifications may be seen) are commonly involved. These may be
out of proportion to the degree of involvement of the vertebra
or disc. Abscesses may also be seen in the paraspinal region and
epidural space. The abscesses are usually located ventrally in
the cervical and lumbar spine and posteriorly in the dorsal
spine. The leptomeninges may be involved. Intraosseus abscesses
may be seen. The abscesses are invariably seen to have a centre
which is isointense to hypointense to normal muscle with a
slightly hyperintense rim on the T1W images. On the T2W images
the centre is hyperintense and the rim hypointense. Contrast
enhancement of the rim is noted. These lesions usually yield
drainable pus. It may be difficult to distinguish phlegmon
(inflammatory mass of granulation tissue) from an abscess.
Phlegmon usually shows diffuse contrast enhancement. This
inflammatory tissue may tunnel beneath the paraspinous
ligaments.
·
The end-stage shows narrowing of the disc space or partial or
complete obliteration with fusion of the vertebral bodies. The
soft tissue components usually regress. The vertebral body may
show central or anterior wedging with gibbus formation.
Hyperintense signal on the T1W images may reflect the presence
of fatty changes or yellow marrow, the result of healing.
Sclerotic changes (hypointense) may be seen. |