|
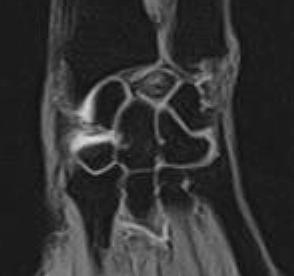
The lunate
carpal bone appears hypointense on the T1 Weighted images and
heterogeneously hyperintense on the GRASS images. There is
slight decrease in the height of the lunate bone with slight
elongation of the lunate in it's antero-posterior dimension.
Fluid is noted in the region of the scaphoid and trapezium
bones.
Lunate
osteonecrosis (Kienböck's disease) may present with wrist pain
and/or loss of grip strength. It is usually seen in men between
the ages of 18 and 40 years. 95% of patients have a history of
heavy manual labor.
Staging
and MRI Findings:
Stage I:
Conventional
radiographs are usually normal in stage I However, a fracture
line or compression fracture may be present. Bone scintigraphy
though sensitive, is nonspecific. On MRI, it is possible to
characterize the extent of necrosis and the morphology of marrow
involvement and of the lunate cortical surfaces, including
articular cartilage. Focal or diffuse hypointensities are seen
on T1W images within the marrow. On T2W or STIR images, the
lunate may show areas of increased signal intensity (hyperemia
or vascular dilation). Unaffected marrow is isointense to normal
marrow. Joint effusions or localized synovitis is hyperintense
on T2W, GRASS or STIR images. Intravenous gadolinium with
fat-suppression displays hyperemic bone with increased signal
intensity.
Stage II:
Conventional
radiographs show sclerosis of the lunate which corresponds to
the hypointense areas on T1W images. Edema, granulation tissue
and areas of preserved vascularity are hyperintense on T2W
images. Usually, the morphology and size are preserved. However,
a decrease in the height of the radial aspect of the lunate may
be seen in late stage II disease.
Stage III:
There is a
distal-to-proximal collapse in the coronal plane and elongation
in the sagittal plane with proximal migration of the capitate.
The absence or presence of scapho-lunate dissociation with
rotatory subluxation of the scaphoid divides patients into IIIA
and IIIB, respectively. Rotation of the scaphoid may be
accompanied by ulnar deviation of the triquetrum. Articular
cartilage degeneration may be seen. Carpal fusions may occur.
Stage IV:
There is
degenerative arthrosis of the lunate and carpus. Hyperintense
areas are not seen on the T2W, GRASS or STIR images and lunate
collapse can be seen in all planes. Splaying of the volar and
dorsal poles of the lunate is accompanied by extrinsic
effacement and convex bowing of the flexor tendons in the
sagittal plane. This may contribute to symptoms of carpal tunnel
syndrome, especially if there is associated proximal migration
of the flexor retinaculum with wrist shortening. Fragmented
portions of the lunate usually demonstrate low signal intensity
on T1W and GRASS images. Synovitis and radiocarpal effusion may
be seen. Pannus tissue is low to intermediate in signal
intensity on T1W and T2W images and enhances with gadolinium
intravenous contrast. There may be wrist arthrodesis. |